Dịch tễ học
Các tỷ lệ ước tính 12 tháng của Rối loạn lo âu lan tỏa [GAD (Generalized Anxiety Disorder)] khoảng từ 1-4% và tỷ lệ mắc suốt đời là khoảng 6% [1,2,3,18]. GAD thường gặp hơn ở người da trắng so với các nhóm khác [19]. Độ tuổi bình thường khởi phát khác nhau và có thể là hai mươi mốt với tuổi trung phát bệnh là khoảng 31 năm [1] và trung bình tuổi phát bệnh là 32,7 năm [20]. Sự phổ biến của GAD được ước tính là 3% ở trẻ em và 10,8% ở thanh thiếu niên [21], với tuổi phát bệnh cho trẻ em và thanh thiếu niên đang ở độ tuổi từ 10 và 14 [22]. Một số dữ liệu cho thấy rằng, phụ nữ có thể có khả năng bị GAD gấp 2-3 lần nhiều hơn nam giới [3,23], và GAD có thể được phổ biến hơn ở người lớn tuổi [24,25]. Rối loạn này được báo cáo thường xuyên không ghi nhận đầy đủ với ít hơn một phần ba số bệnh nhân được điều trị thích đáng [26,27]. Vấn đề này phức tạp hơn ở trẻ em, vì các chỉ định trước của Rối loạn lo âu tuổi thơ và sự khác biệt trong thời thơ ấu của GAD trẻ em so với GAD người lớn.
GAD được kết hợp với giảm chức năng [4,26,28], nghề nghiệp [26], và giảm sút chất lượng cuộc sống [4,26], cũng như chi phí đáng kể về kinh tế [26,29]. Ngoài ra, trong chăm sóc ban đầu, 60-94% bệnh nhân GAD báo cáo triệu chứng cơ thể đau đớn [30,31], và đây là những lý do chính để thăm khám với bác sĩ trong 72% các trường hợp [31].
Bệnh kết hợp
GAD được kèm với tỷ lệ cao của bệnh lý tâm thần bao gồm cả rối loạn lo âu khác hoặc các rối loạn liên quan và Rối loạn trầm cảm nặng [ MDD (Major depressive disorder)] [4]. Các nguy cơ của điều kiện y tế cũng được gia tăng [4], trong đó có hội chứng đau [4,32], tăng huyết áp [4], cũng như các rối loạn tim mạch và dạ dày [4,33]. Sự hiện diện của bệnh trầm cảm kèm theo làm tăng mức độ nghiêm trọng của bệnh, chức năng suy giảm [34], và chi phí kinh tế [29].
Chẩn đoán
GAD được đặc trưng bởi sự lo lắng quá mức và lo lắng về nhiều sự kiện hoặc các hoạt động như trường học hay công việc khó khăn, điều này là rõ ràng trong phần lớn các ngày trong sáu tháng trước đó (Bảng 22) [5]. Ngoài ra, GAD được kết hợp với bồn chồn, căng cơ, mệt mỏi, khó tập trung, dễ bị kích thích, và các vấn đề về giấc ngủ [5].
Bảng 22 Chẩn đoán GAD của DSM-5
• lo âu quá mức và lo lắng (kỳ vọng sợ hãi) về một số sự kiện hoặc hoạt động (ví dụ, trường học / hiệu suất làm việc)
• Các cá nhân khó khăn tìm thấy sự kiểm soát lo lắng
• lo âu quá mức và lo lắng có liên quan với ≥3 các triệu chứng sau đây (với ít nhất là một số xảy ra nhiều ngày trong ≥6 tháng):
○ Bồn chồn hoặc cảm giác căng thẳng hoặc bên bờ vực, dễ dàng mệt mỏi, khó tập trung, dễ cáu kỉnh, căng cơ, hoặc rối loạn giấc ngủ
• Sự rối loạn gây đau khổ đáng kể trên lâm sàng hoặc suy giảm chức năng
Adapted from DSM-5 [5].
Katzman et al. BMC Psychiatry 2014 14(Suppl 1):S1 doi:10.1186/1471-244X-14-S1-S1
Tiêu chuẩn chẩn đoán cho GAD trải qua một sửa đổi nhỏ trong DSM-5 [5] so với DSM-IV-TR [144], yêu cầu rằng những xáo trộn không xảy ra đặc hiệu trong một rối loạn cảm xúc, rối loạn tâm thần, hoặc rối loạn phát triển lan tỏa đã được loại trừ. Tuy nhiên, điều quan trọng vẫn là cần lưu ý rằng, hầu hết các dữ liệu điều trị được mô tả trong phần này được dựa trên các bệnh nhân đáp ứng tiêu chuẩn DSM-IV (hoặc cũ hơn).
Điều trị tâm lý
Phương pháp phân tích tổng hợp chứng minh rõ ràng rằng, liệu pháp nhận thức hành vi [CBT (Cognitive behavioral therapy)] làm giảm đáng kể các triệu chứng GAD và hiệu quả rõ rệt hơn giả dược hoặc danh sách mong đợi kiểm soát các rối loạn của GAD (Level 1) [6,7,8,9,35]. Một vài nghiên cứu đã so sánh CBT và hóa dược đơn độc trong các thử nghiệm tương tự, nhưng mức độ lợi ích xuất hiện có thể so sánh với cả hai nhóm [36-38]. Liệu pháp cá nhân và liệu pháp nhóm xuất hiện với hiệu quả như nhau trong việc làm giảm triệu chứng lo âu, nhưng trị liệu cá nhân có thể dẫn đến cải thiện sớm các triệu chứng lo lắng và trầm cảm [8,35].
Cường độ của liệu pháp điều trị được đánh giá trong một phân tích tổng hợp của 25 nghiên cứu [8]. Các phác đồ bao gồm ít hơn tám phiên bản là hiệu quả như nhau hoặc nhiều hơn với các triệu chứng lo âu, nhưng phác đồ mạnh hơn là hiệu quả hơn trong việc cải thiện các triệu chứng lo lắng và trầm cảm so với các phiên bản yếu hơn[8].
Một số nghiên cứu đã chứng minh, những tiện ích của các chương trình CBT trên internet hoặc CBT dựa trên máy tính [10,39-41]. CBT đã thể hiện được hiệu quả nhiều hơn đáng kể hơn so với những mong đợi kiểm soát [10,39,40], với lợi ích được duy trì ở thời gian dài tiếp theo [40]. Ngoài ra, một chương trình tự nhận thức ngang bằng có hiệu quả như điều trị bình thường, với giảm nhu cầu tiếp xúc cho các bác sĩ chuyên khoa [42].
Một phân tích tổng hợp của năm thử nghiệm cho thấy, không có sự khác biệt đáng kể giữa CBT và liệu pháp thư giãn [6]. Tuy nhiên, các nghiên cứu gần đây cho thấy thư giãn ứng dụng đã hạn chế hiệu quả [43-45]. Một nghiên cứu thực nghiệm lâm sàng [RCT (Research of Clinical Trial)] tìm thấy ít bằng chứng bệnh nhân bị GAD có thể học cách thư giãn trong điều trị hoặc giảm kích hoạt có liên quan với giảm lo âu [44]. Liệu pháp Balneo, một liệu pháp thư giãn liên quan đến phương pháp điều trị spa-related, chứng minh tiềm năng lợi thế hơn liệu pháp hóa dược SSRI trong việc cải thiện điểm số lo âu và tỷ lệ đáp ứng ở bệnh nhân GAD trong một RCT lớn [46].
Chấp nhận điều trị dựa trên hành vi [48], liệu pháp tự nhận thức [43,49], CBT nhắm mục tiêu không khoan dung của sự không chắc chắn [45], và bổ trợ bằng liệu pháp nhận thức chánh niệm [MBCT (Mindfulness-Based Cognitive Therapy)] [16] đã chứng minh hiệu quả trong điều trị GAD.
Liệu pháp tâm lý cũng có thể có lợi, tuy nhiên các kết quả nghiên cứu cho đến nay vẫn chưa rõ ràng. Một RCT cho thấy, trị liệu tâm lý ngắn hạn là hiệu quả như CBT trong việc cải thiện điểm số lo lắng, nhưng CBT là các biện pháp tốt hơn cho lo âu và trầm cảm [52]. Một nghiên cứu khác cho thấy, không có sự khác biệt đáng kể giữa liệu pháp tâm lý ngắn, hóa dược, hoặc sự kết hợp [38].
Không có lợi ích đáng kể nào được tìm thấy với việc bổ sung các liệu pháp xử lý các cá nhân và cảm xúc với CBT khi so sánh với CBT phối hợp[53]. Tuy nhiên, phỏng vấn động lực trước điều trị như là một hỗ trợ cho CBT đã được chứng minh là giúp làm giảm sức đề kháng với điều trị, cải thiện sự tuân thủ bài tập về nhà, và cải thiện kết quả lo lắng - chiến lược này có thể đặc biệt hữu ích trong trường hợp nghiêm trọng hơn [54,55].
Trong thực hành lâm sàng, phương pháp tiếp cận có thể cần phải được cá nhân hóa cho các trãi nghiệm của bệnh nhân.
Điều trị tâm lý và hóa dược
Rất ít dữ liệu có sẵn trong việc sử dụng kết hợp điều trị tâm lý và hóa dược. Một phân tích kết luận rằng, sự kết hợp dược và CBT hiệu quả hơn CBT một mình sau điều trị nhưng không phải trong sáu tháng tiếp theo [11]. So sánh với hóa dược đơn độc, một vài nghiên cứu đã đánh giá những lợi ích của tâm lý trị liệu bổ trợ đã có mâu thuẫn [16,38,56,57]. Một nghiên cứu cho thấy những lợi ích của sự kết hợp [16], trong khi hai nghiên cứu khác đã không có [38,56]. Tuy nhiên, CBT hỗ trợ đã được chỉ ra việc tạo điều kiện giảm dùng benzodiazepine ở bệnh nhân GAD [57].
Không có bằng chứng hiện tại để hỗ trợ sự kết hợp thường xuyên của CBT và hóa dược. Tuy nhiên, trong rối loạn lo âu khác và các rối loạn liên quan, khi bệnh nhân không được hưởng lợi từ CBT hoặc có một phản ứng hạn chế, một thử nghiệm của hóa dược được khuyến khích. Tương tự như vậy, bệnh nhân thấy lợi ích hạn chế từ hóa dược có thể được hưởng lợi từ CBT.
Ảnh hưởng lâu dài của việc điều trị tâm lý
Theo dõi dữ liệu dài hạn từ một phân tích tổng hợp [35] và RCT [38,40,50,58] cho thấy, lợi ích của phương pháp điều trị tâm lý được duy trì ở mức 1-3 năm theo dõi sau điều trị.
Điều trị hóa dược
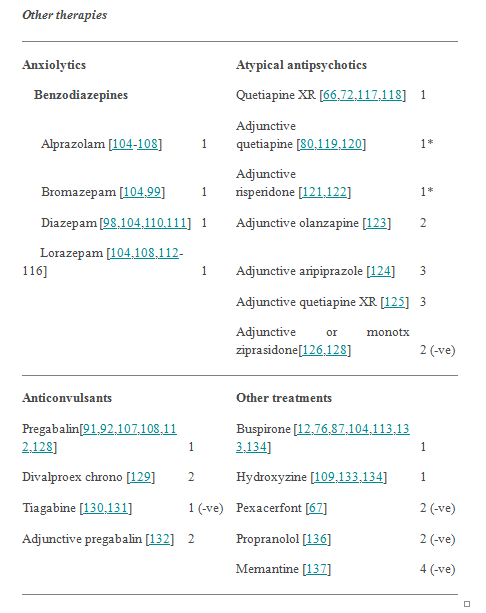
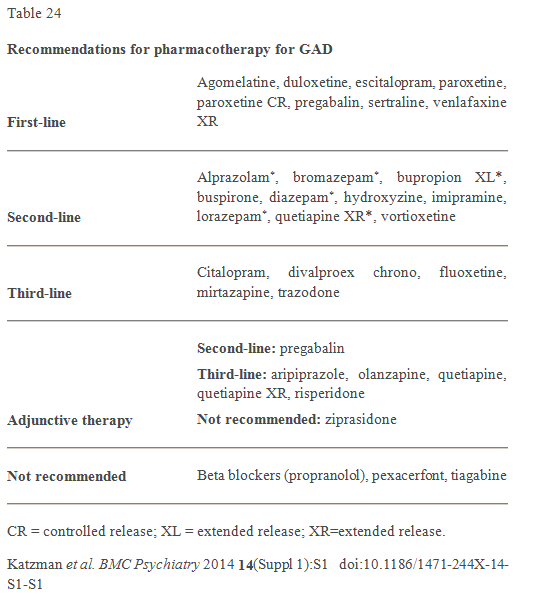
Việc quản lý bệnh nhân GAD nên thực hiện theo các nguyên tắc thảo luận trong phần 2, can thiệp hóa dược có bằng chứng tốt về hiệu quả trong việc điều trị GAD bao gồm SSRIs, SNRIs, TCAs, benzodiazepines, pregabalin, quetiapine XR, và các thuốc khác. Phương pháp điều trị đã được nghiên cứu để sử dụng trong GAD đã được đánh giá theo các tiêu chí độ mạnh của bằng chứng (Bảng 1 và 2) và được tóm tắt trong Bảng 23 và 24.
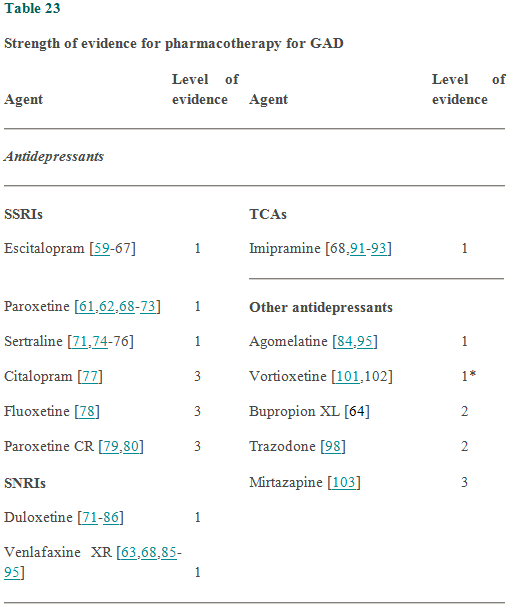
*Conflicting data. SNRI = serotonin–norepinephrine reuptake inhibitor; SSRI = selective serotonin reuptake inhibitor; TCA = tricyclic antidepressant; XL = extended release; XR=extended release; (-ve) = negative.
Katzman et al. BMC Psychiatry 2014 14(Suppl 1):S1 doi:10.1186/1471-244X-14-S1-S1
Thuốc hàng thứ nhất
Thuốc chống trầm cảm (SSRIs & SNRIs): Bằng chứng từ RCT hỗ trợ sử dụng SSRIs bao gồm escitalopram [59-67] và sertraline [71,74-76], cũng như các duloxetine SNRIs [80-86] và venlafaxine XR [63,68,70-95] ( tất cả mức 1) trong điều trị hàng đầu của GAD. Bằng chứng tương tự tồn tại cho paroxetine [61,62,68-73] hỗ trợ việc sử dụng nó như là một lựa chọn hàng đầu. Paroxetin CR có một thành phần hoạt chất tương tự, và mặc dù có ít dữ liệu hỗ trợ việc sử dụng nó, nó có khả năng hoán đổi cho nhau với paroxetine như một thuốc hàng thứ nhất (mức 3) [74,75]. Trong so sánh trực tiếp, hiệu quả của các thuốc SSRI và SNRIs xuất hiện tương tự như nhau [61,62,64,71,85,86]. Một số dữ liệu cho thấy, escitalopram có thể ít hiệu quả hơn so với venlafaxine XR [63] hoặc quetiapine XR [66]. Hiệu quả của venlafaxin tương tự như pregabalin trong một RCT [91], nhưng ít hiệu quả trong một nghiên cứu khác [92].
Thuốc chống trầm cảm khác: Trong hai RCT 12 tuần, mù đôi có đối chứng, agomelatine đã được tìm thấy là hiệu quả hơn giả dược (mức 1) [99,100], và có hiệu quả như escitalopram [100].
Pregabalin: Các thuốc chống co giật pregabalin có hiệu quả hơn giả dược trong RCT [91,92,107,108,112,128] và hiệu quả như benzodiazepines [107,108,112] ở bệnh nhân GAD (mức 1). Pregabalin có hiệu quả hơn venlafaxine XR trong một RCT [92], nhưng tương đương trong một cái khác [91].
Thuốc hàng thứ hai
Benzodiazepines: alprazolam [104-108], Bromazepam [113,115], diazepam [98,114,110,111], và lorazepam [104,108,112-116] tất cả đã chứng minh hiệu quả trong điều trị GAD (mức 1). Trong khi các chất có mức 1 bằng chứng cho hiệu quả, chúng được khuyến cáo như là liệu pháp hàng thứ hai, và thường chỉ sử dụng ngắn hạn, vì tác dụng phụ, phụ thuộc, và các vấn đề cai thuốc.
TCAs và thuốc chống trầm cảm khác: Trong các RCT, imipramine là vượt trội so với giả dược và hiệu quả như benzodiazepines để điều trị GAD (mức 1) [68,96-98]. Tuy nhiên, do tác dụng phụ và độc tính tiềm tàng trong quá liều, imipramine được khuyến cáo như là một lựa chọn thứ hai. Trong khi có rất ít dữ liệu trên bupropion XL (mức 2), trong một RCT 12 tuần ở bệnh nhân GAD, nó là hiệu quả như escitalopram (một lựa chọn hàng đầu), hỗ trợ việc sử dụng nó như là một tùy chọn hàng thứ hai [64].
Vortioxetine là một cái gọi là "serotonin modulator" vì các hoạt động của nó trong một loạt các thụ thể serotonin. Kết quả từ hai RCT tương tự, tám tuần, có đối chứng giả dược được kiểm soát với vortioxetine đã mâu thuẫn nhau, với một thử nghiệm là dương tính [102] và cái khác âm tính (mức 1, mâu thuẫn) [101]. Sự khác biệt trong kết quả có thể liên quan đến sự khác biệt trong tuyển dụng giữa hai nghiên cứu [138], và các dữ liệu cho thấy vortioxetine có thể hữu ích trong GAD.
Quetiapine XR: Có bằng chứng tốt về hiệu quả của quetiapine XR cho việc quản lý của GAD (mức 1) [66,72,117,118]. Hai phân tích tổng hợp [13,14] kết luận rằng quetiapine là cao hơn đáng kể với giả dược và tương đương với thuốc chống trầm cảm [13] để điều trị GAD. Tuy nhiên, quetiapine gây tăng cân và an thần, và tỷ lệ học sinh bỏ học cao hơn do tác dụng phụ so với giả dược hoặc thuốc chống trầm cảm [13,14]. Do khả năng dung nạp và mối quan tâm an toàn lâu dài với thuốc chống loạn thần không điển hình, điều trị này được khuyến cáo như là một tùy chọn hàng thứ hai cho những bệnh nhân không thể dùng thuốc chống trầm cảm hoặc các thuốc benzodiazepin.
Phương pháp điều trị khác: Buspiron hiệu quả hơn giả dược và hiệu quả như các benzodiazepin trong vài RCT (mức 1) [12,76,87,104,113,133,134]. Có ít dữ liệu so sánh buspirone với thuốc chống trầm cảm, là kém hiệu quả hơn so với venlafaxine XR trong một nghiên cứu [87], nhưng hiệu quả như sertraline trong một nghiên cứu khác [76].
Hydroxyzine đã chứng minh hiệu quả vượt trội so với giả dược và tương tự như benzodiazepines và buspirone trong RCT (mức 1) [109,134,135]; Tuy nhiên, kinh nghiệm lâm sàng với các chất này trong việc điều trị GAD còn hạn chế.
Thuốc hàng thứ ba
Các chất sau đây được khuyến cáo như là lựa chọn thứ ba vì dữ liệu hạn chế, tác dụng phụ, hoặc thiếu kinh nghiệm lâm sàng như một liệu pháp chính để điều trị GAD.
Thuốc chống trầm cảm: Trong các nghiên cứu mở hoặc hàng loạt trường hợp, các thuốc chống trầm cảm citalopram [77], fluoxetine [78], paroxetine CR [79,80], và mirtazapine [103] đã chứng minh hiệu quả ở bệnh nhân GAD (tất cả mức 3). Trong một nghiên cứu ngẫu nhiên, trazodone là hiệu quả như diazepam (mức 2) [98].
Phương pháp điều trị khác: chrono divalproex trội hơn giả dược trong điều trị GAD (mức 2) [129], tuy nhiên, công thức này không phải là phổ biến rộng rãi.
Điều trị hỗ trợ
Chiến lược phụ trợ nói chung đã được nghiên cứu ở những bệnh nhân đã có một phản ứng không đủ để điều trị SSRI, và có thể được xem xét cho những bệnh nhân bị GAD kháng trị.
Liệu pháp bổ trợ hàngthứ hai: pregabalin phụ trợ chứng minh hiệu quả tốt trong một RCT lớn ở bệnh nhân GAD người đã có một phản ứng không đủ trước điều trị (Level 2) [132].
Liệu pháp bổ trợ hàng thứ ba: Một phân tích tổng hợp của năm RCT các thuốc chống loạn thần không điển hình bổ trợ không thấy, có sự cải thiện đáng kể trong tỷ lệ đáp ứng cao hơn nhưng tỉ lệ gián đoạn cao so với giả dược ở bệnh nhân GAD dai dẳng [14].
Hai RCT cho thấy rằng, bổ trợ risperidone (mức 1, mâu thuẫn) [121,122] có thể hữu ích trong một số bệnh nhân, nhưng trong RCT lớn hơn nó đã chứng minh tính ưu việt so với giả dược chỉ ở những bệnh nhân có các triệu chứng vừa đến nghiêm trọng [122]. Tương tự như vậy, số liệu về quetiapine bổ trợ đã không phù hợp (mức 1, mâu thuẫn) [80,119,120], với một RCT là âm [80], trong khi RCT khác, không mù RCT cho thấy một số, nhưng lợi ích hạn chế [120]. Olanzapine phụ trợ chứng minh hiệu quả trong một RCT nhỏ ở những bệnh nhân có triệu chứng vẫn còn sau sáu tuần điều trị bằng SSRI [123]. Điều trị phụ trợ với quetiapine XR [125] hoặc aripiprazole [124] (cả hai mức 3) cũng đã có một số lợi ích trong các thử nghiệm mở.
Bởi vì các bằng chứng hạn chế về hiệu quả và tiềm năng của chúng trong tăng cân và tác dụng phụ trao đổi chất, thuốc chống loạn thần không điển hình nên được dành cho những trường hợp điều trị các GAD dai dẳng, và khác với quetiapine XR, chỉ được sử dụng như một điều trị bổ trợ.
Không đề xuất phương pháp điều trị bổ trợ: ziprasidone không xuất hiện để có hiệu quả điều trị hỗ trợ (Level 2, tiêu cực) [126].
Không đề xuất
Propranolol [136] và pexacerfont [67] (cả mức 2, tiêu cực) đã không chứng minh được tính hiệu quả và không nên dùng trong điều trị GAD. Trong khi một thử nghiệm ngẫu nhiên, mở cỡ nhỏ cho rằng tiagabine là hiệu quả như paroxetin, kết quả của ba RCT kiểm soát giả dược không hỗ trợ hiệu quả của tiagabine ở bệnh nhân GAD (mức 1, tiêu cực) [130,131]. Memantine cũng không xuất hiện để có hiệu quả trong rối loạn này (mức 4, tiêu cực) [137].
Điều trị hóa dược duy trì
Điều trị dài hạn được đánh giá trong nghiên cứu theo dõi tự nhiên và ngăn ngừa tái phát. Nghiên cứu phòng tái phát là những người trong đó đáp ứng với điều trị SSRI được chọn ngẫu nhiên để tiếp tục điều trị tích cực hoặc giả dược. Một phân tích của ba nghiên cứu phòng chống tái phát bao gồm 1342 bệnh nhân GAD và tìm thấy sự giảm rất đáng kể trong tỷ lệ tái phát với điều trị SSRI tiếp tục so với giả dược trên sáu đến 12 tháng (tỷ số chênh tái phát là 0,20) [17].
Trong các nghiên cứu RCT ngưng thuốc, duloxetine [139], escitalopram [140], paroxetine [141], và venlafaxine XR [142] đã chứng minh tỷ lệ tái phát thấp hơn đáng kể so với sáu đến 18 tháng trong khoảng từ 10-20% với điều trị tích cực so với 40-56% với giả dược. Pregabalin [143] và quetiapine XR [144] cũng đã chứng minh tỷ lệ tái phát thấp hơn đáng kể so với sáu đến 12 tháng tiếp tục điều trị trong các thử nghiệm ngưng thuốc.
Trong các nghiên cứu dài hạn RCT, escitalopram [61], paroxetine [61], và venlafaxine XR [93,94] đã chứng minh tiếp tục cải thiện so với giả dược trong khoảng sáu tháng
Liệu pháp sinh học và thay thế
Nói chung, các liệu pháp này có thể hữu ích cho một số bệnh nhân; Tuy nhiên, nhiều dữ liệu hơn là cần thiết.
Liệu pháp sinh học: Trong một thử nghiệm mở nhỏ, kích thích từ xuyên sọ lặp lại [TMS (Repetitive Transcranial Magnetic Stimulation) là hiệu quả như đơn trị liệu hoặc như là một thuốc hỗ trợ cho SSRIs ở bệnh nhân GAD (mức 3) [145], và cải thiện được duy trì phần lớn sau sáu tháng khi điều trị [146].
Liệu pháp thay thế: Một số dược thảo đã chứng minh hiệu quả so sánh với lorazepam để điều trị GAD bao gồm silexan (dầu hoa oải hương) (Level 1) [115,147] và chất Galphimia glauca chiết xuất (Level 2) [116]. Phân tích tổng hợp Cochrane tìm thấy hai nghiên cứu của Passiflora (niềm đam mê hoa) cho biết nó là hiệu quả như benzodiazepines (Level 2) [148], và một nghiên cứu của valerian mà thấy không có sự khác biệt đáng kể giữa giả dược, valerian, hoặc diazepam (Level 2, tiêu cực ) [149,150]. Thật không may, bởi vì các chế phẩm này là kém tiêu chuẩn hóa và có sự thay đổi đáng kể trong tỷ lệ của các thành phần hoạt chất trong các sản phẩm khác nhau, chúng có thể không được khuyến cáo rộng rãi.
Một RCT đào tạo phối hợp đối kháng (cử tạ) hay tập thể dục aerobic tìm thấy sự cải thiện triệu chứng đáng kể so với những mong đợi kiểm soát (Level 2) [151]. Một tổng quan hệ thống bao gồm bốn nghiên cứu của châm cứu trong GAD hay lo âu loạn thần kinh, và trong khi tất cả các thử nghiệm báo cáo kết quả tích cực, chi tiết về phương pháp không có và các tác giả kết luận rằng không có đủ bằng chứng để xác định hiệu quả (Level 2) [152]. Nghiên cứu mở cho rằng thiền bổ trợ và điều trị yoga dựa trên có thể hữu ích ở những bệnh nhân với GAD (Level 3) [153,154].
Không đề xuất liệu pháp thay thế: Trong một nghiên cứu ngẫu nhiên, không có sự cải thiện đáng kể với liệu pháp ánh sáng so với giả dược (Level 2, tiêu cực) [155], và điều trị này không được khuyến cáo.
Tóm lược
Tỷ lệ mắc suốt đời của GAD là khoảng 6%, nó có tần suất cao hơn ở phụ nữ so với nam giới, độ tuổi khởi phát phản ánh một phân phối có hai đỉnh (khởi phát vào cuối tuổi thiếu niên đến đầu tuổi hai mươi, và một lần nữa vào những năm 30 và 40). GAD được gắn liền với suy giảm chức năng đáng kể và một tỷ lệ cao của các rối loạn tâm thần và cơ thể kèm theo. Theo tiêu chuẩn DSM-5, GAD được đặc trưng bởi sự lo lắng quá mức và lo lắng về nhiều tình huống và được kết hợp với bồn chồn, căng cơ, và thay đổi hành vi.
CBT là một lựa chọn hàng đầu tiên có hiệu quả trong điều trị GAD và có hiệu quả như hóa dược. CBT dựa trên Internet và dựa trên máy tính cũng đã chứng minh hiệu quả. Bằng chứng không hỗ trợ sự kết hợp thường xuyên của CBT và hóa dược, nhưng khi bệnh nhân không được hưởng lợi từ CBT, một thử nghiệm của hóa dược được khuyến khích, và ngược lại.
Phương pháp tiếp cận hóa dược nên bắt đầu với một trong các tùy chọn hàng thứ nhất bao gồm một SSRI như escitalopram, paroxetine, sertraline hay, một SNRI như duloxetine hay venlafaxine XR, hoặc thuốc chống trầm cảm khác như agomelatine. Các pregabalin chống co giật cũng là một liệu pháp hàng thứ nhất khuyến khích.
Nếu đáp ứng với liều tối ưu là không đầy đủ hoặc các tác nhân không dung nạp được, điều trị nên được chuyển sang một thuốc hàng thứ nhất khác trước khi xem xét các thuốc hàng thứ hai. Sự lựa chọn hàng thứ hai bao gồm bupropion XL, buspirone, hydroxyzine, imipramine, quetiapine XR, vortioxetine, cũng như các benzodiazepin, alprazolam, Bromazepam, diazepam, lorazepam.
Những bệnh nhân không đáp ứng với nhiều quá trình điều trị được coi là có bệnh điều trị dai dẳng. Ở những bệnh nhân như vậy điều quan trọng là phải đánh giá lại các chẩn đoán và xem xét các rối loạn cơ thể và tâm thần kèm theo có ảnh hưởng đến đáp ứng với điều trị. Thuốc hàng thứ ba, liệu pháp bổ trợ, cũng như phương pháp điều trị sinh học và thay thế có thể hữu ích khi bệnh nhân không đáp ứng với một thử nghiệm điều trị tối ưu của phương pháp điều trị thuốc hàng thứ nhất và thứ hai được sử dụng đơn độc và kết hợp.
Tài liệu tham khảo
1. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE: Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication.
Arch Gen Psychiatry 2005, 62:593-602. 
2. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE: Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication.
Arch Gen Psychiatry 2005, 62:617-627.
3. Sherbourne CD, Sullivan G, Craske MG, Roy-Byrne P, Golinelli D, Rose RD, Chavira DA, Bystritsky A, Stein MB: Functioning and disability levels in primary care out-patients with one or more anxiety disorders.
Psychol Med 2010, 40:2059-2068.
4. Comer JS, Blanco C, Hasin DS, Liu SM, Grant BF, Turner JB, Olfson M: Health-related quality of life across the anxiety disorders: results from the national epidemiologic survey on alcohol and related conditions (NESARC).
J Clin Psychiatry 2011, 72:43-50.
5. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Fifth edition. Washington, DC: American Psychiatric Association; 2013.
6. Siev J, Chambless DL: Specificity of treatment effects: cognitive therapy and relaxation for generalized anxiety and panic disorders.
J Consult Clin Psychol 2007, 75:513-522.
7. Borkovec T, Ruscio A: Psychotherapy for generalized anxiety disorder.
J Clin Psychiatry 2001, 62(Suppl 11):37-42.
discussion 43-35
8. Hunot V, Churchill R, Silva de Lima M, Teixeira V: Psychological therapies for generalised anxiety disorder.
Cochrane Database Syst Rev 2007, CD001848.
9. Hofmann SG, Smits JA: Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials.
J Clin Psychiatry 2008, 69:621-632.
10. Titov N, Andrews G, Johnston L, Robinson E, Spence J: Transdiagnostic Internet treatment for anxiety disorders: a randomized controlled trial.
Behav Res Ther 2010, 48:890-899.
11. Hofmann SG, Sawyer AT, Korte KJ, Smits JA: Is it beneficial to add pharmacotherapy to cognitive-behavioral therapy when treating anxiety disorders? a meta-analytic review.
Int J Cogn Ther 2009, 2:160-175.
12. Chessick CA, Allen MH, Thase M, Batista Miralha da Cunha AB, Kapczinski FF, de Lima MS, dos Santos Souza JJ: Azapirones for generalized anxiety disorder.
Cochrane Database Syst Rev 2006, 3:CD006115.
13. Depping AM, Komossa K, Kissling W, Leucht S: Second-generation antipsychotics for anxiety disorders.
Cochrane Database Syst Rev 2010, CD008120.
14. LaLonde CD, Van Lieshout RJ: Treating generalized anxiety disorder with second generation antipsychotics: a systematic review and meta-analysis.
J Clin Psychopharmacol 2011, 31:326-333.
15. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, text revision (DSM-IV-TR). Fourth edition. Washington, DC: American Psychiatric Association; 2000.
16. Kim YW, Lee SH, Choi TK, Suh SY, Kim B, Kim CM, Cho SJ, Kim MJ, Yook K, Ryu M, et al.:Effectiveness of mindfulness-based cognitive therapy as an adjuvant to pharmacotherapy in patients with panic disorder or generalized anxiety disorder.
Depress Anxiety 2009, 26:601-606.
17. Donovan MR, Glue P, Kolluri S, Emir B: Comparative efficacy of antidepressants in preventing relapse in anxiety disorders - a meta-analysis.
J Affect Disord 2010, 123:9-16.
18. Gwynn RC, McQuistion HL, McVeigh KH, Garg RK, Frieden TR, Thorpe LE: Prevalence, diagnosis, and treatment of depression and generalized anxiety disorder in a diverse urban community.
Psychiatr Serv 2008, 59:641-647.
19. Asnaani A, Richey JA, Dimaite R, Hinton DE, Hofmann SG: A cross-ethnic comparison of lifetime prevalence rates of anxiety disorders.
J Nerv Ment Dis 2010, 198:551-555.
20. Grant BF, Hasin DS, Stinson FS, Dawson DA, June Ruan W, Goldstein RB, Smith SM, Saha TD, Huang B: Prevalence, correlates, co-morbidity, and comparative disability of DSM-IV generalized anxiety disorder in the USA: results from the National Epidemiologic Survey on Alcohol and Related Conditions.
Psychol Med 2005, 35:1747-1759.
21. Albano A, Chorpita B, Barlow D: Childhood anxiety disorders. In Child psychopathology. 2nd edition. Edited by Mash E, Barkley R. New York, NY: Guilford; 2003:279-329.
22. Beesdo K, Pine DS, Lieb R, Wittchen HU: Incidence and risk patterns of anxiety and depressive disorders and categorization of generalized anxiety disorder.
Arch Gen Psychiatry 2010, 67:47-57.
23. Ansseau M, Fischler B, Dierick M, Albert A, Leyman S, Mignon A: Socioeconomic correlates of generalized anxiety disorder and major depression in primary care: the GADIS II study (Generalized Anxiety and Depression Impact Survey II).
Depress Anxiety 2008, 25:506-513.
24. Byers AL, Yaffe K, Covinsky KE, Friedman MB, Bruce ML: High occurrence of mood and anxiety disorders among older adults: the National Comorbidity Survey Replication.
Arch Gen Psychiatry 2010, 67:489-496.
25. Mackenzie CS, Reynolds K, Chou KL, Pagura J, Sareen J: Prevalence and correlates of generalized anxiety disorder in a national sample of older adults.
Am J Geriatr Psychiatry 2011, 19:305-315.
26. Revicki DA, Travers K, Wyrwich KW, Svedsater H, Locklear J, Mattera MS, Sheehan DV, Montgomery S: Humanistic and economic burden of generalized anxiety disorder in North America and Europe.
J Affect Disord 2012, 140:103-112.
27. Baldwin DS, Allgulander C, Bandelow B, Ferre F, Pallanti S: An international survey of reported prescribing practice in the treatment of patients with generalised anxiety disorder.
World J Biol Psychiatry 2012, 13:510-516.
28. Weisberg RB, Beard C, Pagano ME, Maki KM, Culpepper L, Keller MB: Impairment and functioning in a sample of primary care patients with generalized anxiety disorder: results from the primary care anxiety project.
Prim Care Companion J Clin Psychiatry 2010., 12
doi 10.4088/PCC.4009m00890blu
29. Zhu B, Zhao Z, Ye W, Marciniak MD, Swindle R: The cost of comorbid depression and pain for individuals diagnosed with generalized anxiety disorder.
J Nerv Ment Dis 2009, 197:136-139.
30. Romera I, Fernandez-Perez S, Montejo AL, Caballero F, Caballero L, Arbesu JA, Delgado-Cohen H, Desaiah D, Polavieja P, Gilaberte I: Generalized anxiety disorder, with or without co-morbid major depressive disorder, in primary care: prevalence of painful somatic symptoms, functioning and health status.
J Affect Disord 2010, 127:160-168.
31. Garcia-Campayo J, Caballero F, Perez M, Lopez V: Pain related factors in newly diagnosed generalized anxiety disorder patients.
Actas Esp Psiquiatr 2012, 40:177-186.
32. Beesdo K, Hoyer J, Jacobi F, Low NC, Hofler M, Wittchen HU: Association between generalized anxiety levels and pain in a community sample: evidence for diagnostic specificity.
J Anxiety Disord 2009, 23:684-693.
33. Martens EJ, de Jonge P, Na B, Cohen BE, Lett H, Whooley MA: Scared to death? Generalized anxiety disorder and cardiovascular events in patients with stable coronary heart disease:The Heart and Soul Study.
Arch Gen Psychiatry 2010, 67:750-758.
34. Tyrer P, Seivewright H, Johnson T: The Nottingham Study of Neurotic Disorder: predictors of 12-year outcome of dysthymic, panic and generalized anxiety disorder.
Psychol Med 2004, 34:1385-1394.
35. Covin R, Ouimet AJ, Seeds PM, Dozois DJ: A meta-analysis of CBT for pathological worry among clients with GAD.
J Anxiety Disord 2008, 22:108-116.
36. Linden M, Zubraegel D, Baer T, Franke U, Schlattmann P: Efficacy of cognitive behaviour therapy in generalized anxiety disorders. Results of a controlled clinical trial (Berlin CBT-GAD Study).
Psychother Psychosom 2005, 74:36-42.
37. Borkovec T, Newman M, Pincus A, Lytle R: A component analysis of cognitive-behavioral therapy for generalized anxiety disorder and the role of interpersonal problems.
J Consult Clin Psychol 2002, 70:288-298.
38. Ferrero A, Piero A, Fassina S, Massola T, Lanteri A, Daga GA, Fassino S: A 12-month comparison of brief psychodynamic psychotherapy and pharmacotherapy treatment in subjects with generalised anxiety disorders in a community setting.
Eur Psychiatry 2007, 22:530-539.
39. Robinson E, Titov N, Andrews G, McIntyre K, Schwencke G, Solley K: Internet treatment for generalized anxiety disorder: a randomized controlled trial comparing clinician vs. technician assistance.
PLoS One 2010, 5:e10942.
40. Paxling B, Almlov J, Dahlin M, Carlbring P, Breitholtz E, Eriksson T, Andersson G: Guided internet-delivered cognitive behavior therapy for generalized anxiety disorder: a randomized controlled trial.
Cogn Behav Ther 2011, 40:159-173.
41. Gorini A, Pallavicini F, Algeri D, Repetto C, Gaggioli A, Riva G: Virtual reality in the treatment of generalized anxiety disorders.
Stud Health Technol Inform 2010, 154:39-43.
42. den Boer PC, Wiersma D, Ten Vaarwerk I, Span MM, Stant AD, Van den Bosch RJ:Cognitive self-therapy for chronic depression and anxiety: a multi-centre randomized controlled study.
Psychol Med 2007, 37:329-339.
43. Wells A, Welford M, King P, Papageorgiou C, Wisely J, Mendel E: A pilot randomized trial of metacognitive therapy vs applied relaxation in the treatment of adults with generalized anxiety disorder.
Behav Res Ther 2010, 48:429-434.
44. Conrad A, Isaac L, Roth WT: The psychophysiology of generalized anxiety disorder: 2. Effects of applied relaxation.
Psychophysiology 2008, 45:377-388.
45. Dugas MJ, Brillon P, Savard P, Turcotte J, Gaudet A, Ladouceur R, Leblanc R, Gervais NJ: A randomized clinical trial of cognitive-behavioral therapy and applied relaxation for adults with generalized anxiety disorder.
Behav Ther 2010, 41:46-58.
46. Dubois O, Salamon R, Germain C, Poirier MF, Vaugeois C, Banwarth B, Mouaffak F, Galinowski A, Olie JP: Balneotherapy versus paroxetine in the treatment of generalized anxiety disorder.
Complement Ther Med 2010, 18:1-7.
47. Dugas MJ, Marchand A, Ladouceur R: Further validation of a cognitive-behavioral model of generalized anxiety disorder: diagnostic and symptom specificity.
J Anxiety Disord 2005, 19:329-343.
48. Roemer L, Orsillo SM, Salters-Pedneault K: Efficacy of an acceptance-based behavior therapy for generalized anxiety disorder: evaluation in a randomized controlled trial.
J Consult Clin Psychol 2008, 76:1083-1089.
49. van der Heiden C, Muris P, van der Molen HT: Randomized controlled trial on the effectiveness of metacognitive therapy and intolerance-of-uncertainty therapy for generalized anxiety disorder.
Behav Res Ther 2012, 50:100-109.
50. Hoyer J, Beesdo K, Gloster AT, Runge J, Hofler M, Becker ES: Worry exposure versus applied relaxation in the treatment of generalized anxiety disorder.
Psychother Psychosom 2009, 78:106-115.
51. Riskind JH, Williams NL, Joiner TE Jr: The looming cognitive style: A cognitive vulnerability for anxiety disorders.
J Social Clin Psychol 2006, 25:779-801.
52. Leichsenring F, Salzer S, Jaeger U, Kachele H, Kreische R, Leweke F, Ruger U, Winkelbach C, Leibing E: Short-term psychodynamic psychotherapy and cognitive-behavioral therapy in generalized anxiety disorder: a randomized, controlled trial.
Am J Psychiatry 2009, 166:875-881.
53. Newman MG, Castonguay LG, Borkovec TD, Fisher AJ, Boswell JF, Szkodny LE, Nordberg SS: A randomized controlled trial of cognitive-behavioral therapy for generalized anxiety disorder with integrated techniques from emotion-focused and interpersonal therapies.
J Consult Clin Psychol 2011, 79:171-181.
54. Aviram A, Westra HA: The impact of motivational interviewing on resistance in cognitive behavioural therapy for generalized anxiety disorder.
Psychother Res 2011, 21:698-708.
55. Westra HA, Arkowitz H, Dozois DJ: Adding a motivational interviewing pretreatment to cognitive behavioral therapy for generalized anxiety disorder: a preliminary randomized controlled trial.
J Anxiety Disord 2009, 23:1106-1117.
56. Crits-Christoph P, Newman MG, Rickels K, Gallop R, Gibbons MB, Hamilton JL, Ring-Kurtz S, Pastva AM: Combined medication and cognitive therapy for generalized anxiety disorder.
J Anxiety Disord 2011, 25:1087-1094.
57. Gosselin P, Ladouceur R, Morin CM, Dugas MJ, Baillargeon L: Benzodiazepine discontinuation among adults with GAD: A randomized trial of cognitive-behavioral therapy.
J Consult Clin Psychol 2006, 74:908-919.
58. Salzer S, Winkelbach C, Leweke F, Leibing E, Leichsenring F: Long-term effects of short-term psychodynamic psychotherapy and cognitive-behavioural therapy in generalized anxiety disorder: 12-month follow-up.
Can J Psychiatry 2011, 56:503-508.
59. Davidson J, Bose A, Korotzer A, Zheng H: Escitalopram in the treatment of generalized anxiety disorder: double-blind, placebo controlled, flexible-dose study.
Depress Anxiety 2004, 19:234-240.
60. Goodman WK, Bose A, Wang Q: Treatment of generalized anxiety disorder with escitalopram: pooled results from double-blind, placebo-controlled trials.
J Affect Disord 2005, 87:161-167.
61. Bielski RJ, Bose A, Chang CC: A double-blind comparison of escitalopram and paroxetine in the long-term treatment of generalized anxiety disorder.
Ann Clin Psychiatry 2005, 17:65-69.
62. Baldwin DS, Huusom AK, Maehlum E: Escitalopram and paroxetine in the treatment of generalised anxiety disorder: randomised, placebo-controlled, double-blind study.
Br J Psychiatry 2006, 189:264-272.
63. Bose A, Korotzer A, Gommoll C, Li D: Randomized placebo-controlled trial of escitalopram and venlafaxine XR in the treatment of generalized anxiety disorder.
Depress Anxiety 2008, 25:854-861.
64. Bystritsky A, Kerwin L, Feusner JD, Vapnik T: A pilot controlled trial of bupropion XL versus escitalopram in generalized anxiety disorder.
Psychopharmacol Bull 2008, 41:46-51.
65. Lenze EJ, Rollman BL, Shear MK, Dew MA, Pollock BG, Ciliberti C, Costantino M, Snyder S, Shi P, Spitznagel E, et al.: Escitalopram for older adults with generalized anxiety disorder: a randomized controlled trial.
JAMA 2009, 301:295-303.
66. Merideth C, Cutler AJ, She F, Eriksson H: Efficacy and tolerability of extended release quetiapine fumarate monotherapy in the acute treatment of generalized anxiety disorder: a randomized, placebo controlled and active-controlled study.
Int Clin Psychopharmacol 2012, 27:40-54.
67. Coric V, Feldman HH, Oren DA, Shekhar A, Pultz J, Dockens RC, Wu X, Gentile KA, Huang SP, Emison E, et al.: Multicenter, randomized, double-blind, active comparator and placebo-controlled trial of a corticotropin-releasing factor receptor-1 antagonist in generalized anxiety disorder.
Depress Anxiety 2010, 27:417-425.
68. Kapczinski F, Lima MS, Souza JS, Schmitt R: Antidepressants for generalized anxiety disorder.
Cochrane Database Syst Rev 2003, CD003592.
69. Rickels K, Zaninelli R, McCafferty J, Bellew K, Iyengar M, Sheehan D: Paroxetine treatment of generalized anxiety disorder: a double-blind, placebo-controlled study.
Am J Psychiatry 2003, 160:749-756.
70. Pollack M, Zaninelli R, Goddard A, McCafferty J, Bellew K, Burnham D, Iyengar M:Paroxetine in the treatment of generalized anxiety disorder: results of a placebo-controlled, flexible-dosage trial.
J Clin Psychiatry 2001, 62:350-357.
71. Ball S, Kuhn A, Wall D, Shekhar A, Goddard A: Selective serotonin reuptake inhibitor treatment for generalized anxiety disorder: a double-blind, prospective comparison between paroxetine and sertraline.
J Clin Psychiatry 2005, 66:94-99.
72. Bandelow B, Chouinard G, Bobes J, Ahokas A, Eggens I, Liu S, Eriksson H: Extended-release quetiapine fumarate (quetiapine XR): a once-daily monotherapy effective in generalized anxiety disorder. Data from a randomized, double-blind, placebo- and active-controlled study.
Int J Neuropsychopharmacol 2010, 13:305-320.
73. Kim TS, Pae CU, Yoon SJ, Bahk WM, Jun TY, Rhee WI, Chae JH: Comparison of venlafaxine extended release versus paroxetine for treatment of patients with generalized anxiety disorder.
Psychiatry Clin Neurosci 2006, 60:347-351.
74. Allgulander C, Dahl A, Austin C, Morris P, Sogaard J, Fayyad R, Kutcher S, Clary C: Efficacy of sertraline in a 12-week trial for generalized anxiety disorder.
Am J Psychiatry 2004, 161:1642-1649.
75. Brawman-Mintzer O, Knapp RG, Rynn M, Carter RE, Rickels K: Sertraline treatment for generalized anxiety disorder: a randomized, double-blind, placebo-controlled study.
J Clin Psychiatry 2006, 67:874-881.
76. Mokhber N, Azarpazhooh MR, Khajehdaluee M, Velayati A, Hopwood M: Randomized, single-blind, trial of sertraline and buspirone for treatment of elderly patients with generalized anxiety disorder.
Psychiatry Clin Neurosci 2010, 64:128-133.
77. Varia I, Rauscher F: Treatment of generalized anxiety disorder with citalopram.
Int Clin Psychopharmacol 2002, 17:103-107.
78. Simon NM, Zalta AK, Worthington JJ 3rd, Hoge EA, Christian KM, Stevens JC, Pollack MH:Preliminary support for gender differences in response to fluoxetine for generalized anxiety disorder.
Depress Anxiety 2006, 23:373-376.
79. Gross PK, Nourse R, Wasser TE, Krulewicz S: Effects of paroxetine CR on depressive and anxiety symptoms: in a community sample of adult Hispanic women with major depression or generalized anxiety disorder.
Psychiatry (Edgmont) 2006, 3:64-68.
80. Simon NM, Connor KM, LeBeau RT, Hoge EA, Worthington JJ 3rd, Zhang W, Davidson JR, Pollack MH: Quetiapine augmentation of paroxetine CR for the treatment of refractory generalized anxiety disorder: preliminary findings.
Psychopharmacology (Berl) 2008, 197:675-681.
81. Rynn M, Russell J, Erickson J, Detke MJ, Ball S, Dinkel J, Rickels K, Raskin J: Efficacy and safety of duloxetine in the treatment of generalized anxiety disorder: a flexible-dose, progressive-titration, placebo-controlled trial.
Depress Anxiety 2008, 25:182-189.
82. Koponen H, Allgulander C, Erickson J, Dunayevich E, Pritchett Y, Detke MJ, Ball SG, Russell JM: Efficacy of duloxetine for the treatment of generalized anxiety disorder: implications for primary care physicians.
Prim Care Companion J Clin Psychiatry 2007, 9:100-107.
83. Wu WY, Wang G, Ball SG, Desaiah D, Ang QQ: Duloxetine versus placebo in the treatment of patients with generalized anxiety disorder in China.
Chin Med J (Engl) 2011, 124:3260-3268.
84. Allgulander C, Hartford J, Russell J, Ball S, Erickson J, Raskin J, Rynn M: Pharmacotherapy of generalized anxiety disorder: results of duloxetine treatment from a pooled analysis of three clinical trials.
Curr Med Res Opin 2007, 23:1245-1252.
85. Hartford J, Kornstein S, Liebowitz M, Pigott T, Russell J, Detke M, Walker D, Ball S, Dunayevich E, Dinkel J, Erickson J: Duloxetine as an SNRI treatment for generalized anxiety disorder: results from a placebo and active-controlled trial.
Int Clin Psychopharmacol 2007, 22:167-174.
86. Allgulander C, Nutt D, Detke M, Erickson J, Spann M, Walker D, Ball SG, Russell JM: A non-inferiority comparison of duloxetine and venlafaxine in the treatment of adult patients with generalized anxiety disorder.
J Psychopharmacol 2008, 22:417-425.
87. Davidson J, Du Pont R, Hedges D, Haskins J: Efficacy, safety, and tolerability of venlafaxine extended release and buspirone in outpatients with generalized anxiety disorder.
J Clin Psychiatry 1999, 60:528-535.
88. Nimatoudis I, Zissis N, Kogeorgos J, Theodoropoulou S, Vidalis A, Kaprinis G: Remission rates with venlafaxine extended release in Greek outpatients with generalized anxiety disorder. A double-blind, randomized, placebo controlled study.
Int Clin Psychopharmacol 2004, 19:331-336.
89. Rickels K, Pollack M, Sheehan D, Haskins J: Efficacy of extended-release venlafaxine in nondepressed outpatients with generalized anxiety disorder.
Am J Psychiatry 2000, 157:968-974.
90. Katz I, Reynolds C, Alexopoulos G, Hackett D: Venlafaxine ER as a treatment for generalized anxiety disorder in older adults: pooled analysis of five randomized placebo-controlled clinical trials.
J Am Geriatr Soc 2002, 50:18-25.
91.Montgomery SA, Tobias K, Zornberg GL, Kasper S, Pande AC: Efficacy and safety of pregabalin in the treatment of generalized anxiety disorder: a 6-week, multicenter, randomized, double-blind, placebo-controlled comparison of pregabalin and venlafaxine.
J Clin Psychiatry 2006, 67:771-782.
92.Kasper S, Herman B, Nivoli G, Van Ameringen M, Petralia A, Mandel FS, Baldinetti F, Bandelow B: Efficacy of pregabalin and venlafaxine-XR in generalized anxiety disorder: results of a double-blind, placebo-controlled 8-week trial.
Int Clin Psychopharmacol 2009, 24:87-96.
93.Allgulander C, Hackett D, Salinas E: Venlafaxine extended release (ER) in the treatment of generalised anxiety disorder: twenty-four-week placebo-controlled dose-ranging study.
Br J Psychiatry 2001, 179:15-22.
94.Gelenberg A, Lydiard R, Rudolph R, Aguiar L, Haskins J, Salinas E: Efficacy of venlafaxine extended-release capsules in nondepressed outpatients with generalized anxiety disorder: A 6-month randomized controlled trial.
JAMA 2000, 283:3082-3088.
95.Lenox-Smith AJ, Reynolds A: A double-blind, randomised, placebo controlled study of venlafaxine XL in patients with generalised anxiety disorder in primary care.
Br J Gen Pract 2003, 53:772-777.
96. Hoehn-Saric R, McLeod D, Zimmerli W: Differential effects of alprazolam and imipramine in generalized anxiety disorder: somatic versus psychic symptoms.
J Clin Psychiatry 1988, 49:293-301.
97. Rocca P, Fonzo V, Scotta M, Zanalda E, Ravizza L: Paroxetine efficacy in the treatment of generalized anxiety disorder.
Acta Psychiatr Scand 1997, 95:444-450.
98. Rickels K, Downing R, Schweizer E, Hassman H: Antidepressants for the treatment of generalized anxiety disorder. A placebo-controlled comparison of imipramine, trazodone, and diazepam.
Arch Gen Psychiatry 1993, 50:884-895.
99. Stein DJ, Ahokas AA, de Bodinat C: Efficacy of agomelatine in generalized anxiety disorder: a randomized, double-blind, placebo-controlled study.
J Clin Psychopharmacol 2008, 28:561-566.
100. Stein D, Marquez M, Hoschl C, Ahokas A, Oh K-S, Jarema M, Avedisova A, Vavrusova L, Olivier V: Efficacy and tolerability of agomelatine in generalized anxiety disorder: A randomised double blind placebo controlled trial with escitalopram as active control [poster].
28th CINP Congress; Jun 3-7; Stockholm, Sweden 2012.
101. Rothschild AJ, Mahableshwarkar AR, Jacobsen P, Yan M, Sheehan DV: Vortioxetine (Lu AA21004) 5mg in generalized anxiety disorder: Results of an 8-week randomized, double-blind, placebo-controlled clinical trial in the United States.
Eur Neuropsychopharmacol 2012, 22:858-866.
102. Bidzan L, Mahableshwarkar AR, Jacobsen P, Yan M, Sheehan DV: Vortioxetine (Lu AA21004) in generalized anxiety disorder: Results of an 8-week, multinational, randomized, double-blind, placebo-controlled clinical trial.
Eur Neuropsychopharmacol 2012, 22:847-857.
103. Gambi F, De Berardis D, Campanella D, Carano A, Sepede G, Salini G, Mezzano D, Cicconetti A, Penna L, Salerno RM, Ferro FM: Mirtazapine treatment of generalized anxiety disorder: a fixed dose, open label study.
J Psychopharmacol 2005, 19:483-487.
104.Mitte K, Noack P, Steil R, Hautzinger M: A meta-analytic review of the efficacy of drug treatment in generalized anxiety disorder.
J Clin Psychopharmacol 2005, 25:141-150.
105. Lydiard R, Ballenger J, Rickels K: A double-blind evaluation of the safety and efficacy of abecarnil, alprazolam, and placebo in outpatients with generalized anxiety disorder. Abecarnil Work Group.
J Clin Psychiatry 1997, 58(Suppl 11):11-18.
106. Moller H, Volz H, Reimann I, Stoll K: Opipramol for the treatment of generalized anxiety disorder: a placebo-controlled trial including an alprazolam-treated group.
J Clin Psychopharmacol 2001, 21:59-65.
107. Rickels K, Pollack MH, Feltner DE, Lydiard RB, Zimbroff DL, Bielski RJ, Tobias K, Brock JD, Zornberg GL, Pande AC: Pregabalin for treatment of generalized anxiety disorder: a 4-week, multicenter, double-blind, placebo-controlled trial of pregabalin and alprazolam.
Arch Gen Psychiatry 2005, 62:1022-1030.
108. Lydiard RB, Rickels K, Herman B, Feltner DE: Comparative efficacy of pregabalin and benzodiazepines in treating the psychic and somatic symptoms of generalized anxiety disorder.
Int J Neuropsychopharmacol 2010, 13:229-241.
109. Llorca P, Spadone C, Sol O, Danniau A, Bougerol T, Corruble E, Faruch M, Macher J, Sermet E, Servant D: Efficacy and safety of hydroxyzine in the treatment of generalized anxiety disorder: a 3-month double-blind study.
J Clin Psychiatry 2002, 63:1020-1027.
110. Rickels K, Schweizer E, De Martinis N, Mandos L, Mercer C: Gepirone and diazepam in generalized anxiety disorder: a placebo-controlled trial.
J Clin Psychopharmacol 1997, 17:272-277.
111. Rickels K, DeMartinis N, Aufdembrinke B: A double-blind, placebo-controlled trial of abecarnil and diazepam in the treatment of patients with generalized anxiety disorder.
J Clin Psychopharmacol 2000, 20:12-18.
112.Feltner D, Crockatt J, Dubovsky S, Cohn C, Shrivastava R, Targum S, Liu-Dumaw M, Carter C, Pande A: A randomized, double-blind, placebo-controlled, fixed-dose, multicenter study of pregabalin in patients with generalized anxiety disorder.
J Clin Psychopharmacol 2003, 23:240-249.
113. Laakmann G, Schule C, Lorkowski G, Baghai T, Kuhn K, Ehrentraut S: Buspirone and lorazepam in the treatment of generalized anxiety disorder in outpatients.
Psychopharmacology (Berl) 1998, 136:357-366.
114. Fresquet A, Sust M, Lloret A, Murphy M, Carter F, Campbell G, Marion-Landais G: Efficacy and safety of lesopitron in outpatients with generalized anxiety disorder.
Ann Pharmacother 2000, 34:147-153.
115. Woelk H, Schlafke S: A multi-center, double-blind, randomised study of the lavender oil preparation Silexan in comparison to lorazepam for generalized anxiety disorder.
Phytomedicine 2010, 17:94-99.
116.Herrera-Arellano A, Jimenez-Ferrer E, Zamilpa A, Morales-Valdez M, Garcia-Valencia CE, Tortoriello J: Efficacy and tolerability of a standardized herbal product from galphimia glauca on generalized anxiety disorder. A randomized, double-blind clinical trial controlled with lorazepam.
Planta Med 2007, 73:713-717.
117. Khan A, Joyce M, Atkinson S, Eggens I, Baldytcheva I, Eriksson H: A randomized, double-blind study of once-daily extended release quetiapine fumarate (quetiapine XR) monotherapy in patients with generalized anxiety disorder.
J Clin Psychopharmacol 2011, 31:418-428.
118. Stein DJ, Bandelow B, Merideth C, Olausson B, Szamosi J, Eriksson H: Efficacy and tolerability of extended release quetiapine fumarate (quetiapine XR) monotherapy in patients with generalised anxiety disorder: an analysis of pooled data from three 8-week placebo-controlled studies.
Hum Psychopharmacol 2011, 26:614-628.
119. Katzman MA, Vermani M, Jacobs L, Marcus M, Kong B, Lessard S, Galarraga W, Struzik L, Gendron A: Quetiapine as an adjunctive pharmacotherapy for the treatment of non-remitting generalized anxiety disorder: a flexible-dose, open-label pilot trial.
J Anxiety Disord 2008, 22:1480-1486.
120. Altamura AC, Serati M, Buoli M, Dell'Osso B: Augmentative quetiapine in partial/nonresponders with generalized anxiety disorder: a randomized, placebo-controlled study.
Int Clin Psychopharmacol 2011, 26:201-205.
121.Brawman-Mintzer O, Knapp RG, Nietert PJ: Adjunctive risperidone in generalized anxiety disorder: a double-blind, placebo-controlled study.
J Clin Psychiatry 2005, 66:1321-1325.
122.Pandina GJ, Canuso CM, Turkoz I, Kujawa M, Mahmoud RA: Adjunctive risperidone in the treatment of generalized anxiety disorder: a double-blind, prospective, placebo-controlled, randomized trial.
Psychopharmacol Bull 2007, 40:41-57.
123.Pollack MH, Simon NM, Zalta AK, Worthington JJ, Hoge EA, Mick E, Kinrys G, Oppenheimer J: Olanzapine augmentation of fluoxetine for refractory generalized anxiety disorder: a placebo controlled study.
Biol Psychiatry 2006, 59:211-215.
124. Menza MA, Dobkin RD, Marin H: An open-label trial of aripiprazole augmentation for treatment-resistant generalized anxiety disorder [Letter].
J Clin Psychopharmacol 2007, 27:207-210.
125. Gabriel A: The extended-release formulation of quetiapine fumarate (quetiapine XR) adjunctive treatment in partially responsive generalized anxiety disorder (GAD): An open label naturalistic study.
Clin Ter 2011, 162:113-118.
126. Lohoff FW, Etemad B, Mandos LA, Gallop R, Rickels K: Ziprasidone treatment of refractory generalized anxiety disorder: a placebo-controlled, double-blind study.
J Clin Psychopharmacol 2010, 30:185-189.
127. Snyderman SH, Rynn MA, Rickels K: Open-label pilot study of ziprasidone for refractory generalized anxiety disorder [Letter].
J Clin Psychopharmacol 2005, 25:497-499.
128. Pohl R, Feltner D, Fieve R, Pande A: Efficacy of pregabalin in the treatment of generalized anxiety disorder: double-blind, placebo-controlled comparison of BID versus TID dosing.
J Clin Psychopharmacol 2005, 25:151-158.
129. Aliyev NA, Aliyev ZN: Valproate (depakine-chrono) in the acute treatment of outpatients with generalized anxiety disorder without psychiatric comorbidity: randomized, double-blind placebo-controlled study.
Eur Psychiatry 2008, 23:109-114.
130. Pollack MH, Tiller J, Xie F, Trivedi MH: Tiagabine in adult patients with generalized anxiety disorder: results from 3 randomized, double-blind, placebo-controlled, parallel-group studies.
J Clin Psychopharmacol 2008, 28:308-316.
131. Rosenthal M: Tiagabine for the treatment of generalized anxiety disorder: a randomized, open-label, clinical trial with paroxetine as a positive control.
J Clin Psychiatry 2003, 64:1245-1249.
132. Rickels K, Shiovitz TM, Ramey TS, Weaver JJ, Knapp LE, Miceli JJ: Adjunctive therapy with pregabalin in generalized anxiety disorder patients with partial response to SSRI or SNRI treatment.
Int Clin Psychopharmacol 2012, 27:142-150.
133. Pollack M, Worthington J, Manfro G, Otto M, Zucker B: Abecarnil for the treatment of generalized anxiety disorder: a placebo-controlled comparison of two dosage ranges of abecarnil and buspirone.
J Clin Psychiatry 1997, 58(Suppl 11):19-23.
134. Lader M, Scotto J: A multicentre double-blind comparison of hydroxyzine, buspirone and placebo in patients with generalized anxiety disorder.
Psychopharmacology (Berl) 1998, 139:402-406.
135. Guaiana G, Barbui C, Cipriani A: Hydroxyzine for generalised anxiety disorder.
Cochrane Database Syst Rev 2010, CD006815.
136. Meibach RC, Dunner D, Wilson LG, Ishiki D, Dager SR: Comparative efficacy of propranolol, chlordiazepoxide, and placebo in the treatment of anxiety: a double-blind trial.
J Clin Psychiatry 1987, 48:355-358.
137. Feusner JD, Kerwin L, Saxena S, Bystritsky A: Differential efficacy of memantine for obsessive-compulsive disorder vs. generalized anxiety disorder: an open-label trial.
Psychopharmacol Bull 2009, 42:81-93.
138. Baldwin DS, Nutt DJ: On assessing potential efficacy for vortioxetine in generalized anxiety disorder.
Eur Neuropsychopharmacol 2012, 22:841-843.
139. Davidson JR, Wittchen HU, Llorca PM, Erickson J, Detke M, Ball SG, Russell JM: Duloxetine treatment for relapse prevention in adults with generalized anxiety disorder: a double-blind placebo-controlled trial.
Eur Neuropsychopharmacol 2008, 18:673-681.
140. Allgulander C, Florea I, Huusom AK: Prevention of relapse in generalized anxiety disorder by escitalopram treatment.
Int J Neuropsychopharmacol 2006, 9:495-505.
141. Stocchi F, Nordera G, Jokinen R, Lepola U, Hewett K, Bryson H, Iyengar M: Efficacy and tolerability of paroxetine for the long-term treatment of generalized anxiety disorder.
J Clin Psychiatry 2003, 64:250-258.
142. Rickels K, Etemad B, Khalid-Khan S, Lohoff FW, Rynn MA, Gallop RJ: Time to relapse after 6 and 12 months' treatment of generalized anxiety disorder with venlafaxine extended release.
Arch Gen Psychiatry 2010, 67:1274-1281.
143. Feltner D, Wittchen HU, Kavoussi R, Brock J, Baldinetti F, Pande AC: Long-term efficacy of pregabalin in generalized anxiety disorder.
Int Clin Psychopharmacol 2008, 23:18-28.
144. Katzman MA, Brawman-Mintzer O, Reyes EB, Olausson B, Liu S, Eriksson H: Extended release quetiapine fumarate (quetiapine XR) monotherapy as maintenance treatment for generalized anxiety disorder: a long-term, randomized, placebo-controlled trial.
Int Clin Psychopharmacol 2011, 26:11-24.
145. Bystritsky A, Kaplan JT, Feusner JD, Kerwin LE, Wadekar M, Burock M, Wu AD, Iacoboni M:A preliminary study of fMRI-guided rTMS in the treatment of generalized anxiety disorder.
J Clin Psychiatry 2008, 69:1092-1098.
146. Bystritsky A, Kerwin LE, Feusner JD: A preliminary study of fMRI-guided rTMS in the treatment of generalized anxiety disorder: 6-month follow-up [Letter].
J Clin Psychiatry 2009, 70:431-432.
147. Kasper S, Gastpar M, Muller WE, Volz HP, Moller HJ, Dienel A, Schlafke S: Silexan, an orally administered Lavandula oil preparation, is effective in the treatment of 'subsyndromal' anxiety disorder: a randomized, double-blind, placebo controlled trial.
Int Clin Psychopharmacol 2010, 25:277-287.
148. Miyasaka LS, Atallah AN, Soares BG: Passiflora for anxiety disorder.
Cochrane Database Syst Rev 2007, CD004518.
149. Andreatini R, Sartori VA, Seabra ML, Leite JR: Effect of valepotriates (valerian extract) in generalized anxiety disorder: a randomized placebo-controlled pilot study.
Phytother Res 2002, 16:650-654.
150. Miyasaka LS, Atallah AN, Soares BG: Valerian for anxiety disorders.
Cochrane Database Syst Rev 2006, CD004515.
151. Herring MP, Jacob ML, Suveg C, Dishman RK, O'Connor PJ: Feasibility of exercise training for the short-term treatment of generalized anxiety disorder: a randomized controlled trial.
Psychother Psychosom 2012, 81:21-28.
152. Pilkington K, Kirkwood G, Rampes H, Cummings M, Richardson J: Acupuncture for anxiety and anxiety disorders--a systematic literature review.
Acupunct Med 2007, 25:1-10.
153. Lu CF, Smith LN, Gau CH: Exploring the zen meditation experiences of patients with generalized anxiety disorder: a focus-group approach.
J Nurs Res 2012, 20:43-52.
154. Katzman MA, Vermani M, Gerbarg PL, Brown RP, Iorio C, Davis M, Cameron C, Tsirgielis D:A multicomponent yoga-based, breath intervention program as an adjunctive treatment in patients suffering from generalized anxiety disorder with or without comorbidities.
Int J Yoga 2012, 5:57-65.
155. Youngstedt SD, Kline CE, Ginsberg JP, Zielinski MR, Hardin JW: Bright light treatment for high-anxious young adults: a randomized controlled pilot study.
Depress Anxiety 2011, 28:324-332.
Lược dịch: BSCKI. Nguyễn Đăng Nguyên